







It is important to follow the instructions given by your surgeon during the recovery period after surgery for Haglund’s deformity. During the first 10 days, the foot should be kept elevated and should not be supported on the ground. After this period, if the doctor allows it, the patient can start to support the foot with the use of a special boot provided by the clinic. It is essential to attend all scheduled post-operative appointments with the surgeon and to report any abnormal symptoms such as excessive bleeding, severe pain, redness or itching. Following a healthy and balanced diet, taking vitamin C supplements and applying ice to the foot can also help with the recovery process.
The patient must arrive at the clinic at the time they are scheduled. Legal procedures will be carried out before they are taken to the operating room. The patient will then change into a gown provided by the hospital. The doctor will instruct them to lie down on the operating table in the appropriate position. Anesthesia, either general or local, will be administered as planned. The surgery will not take more than 60 minutes. After the surgery, the patient’s foot will be immobilized and covered with a cast. The patient may also be given an injection to alleviate pain before they return home.
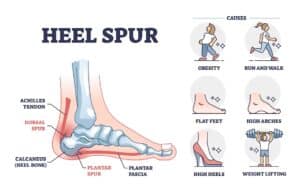
Some physical conditions or health issues can be risk factors for Haglund’s deformity, including:
- Wearing tight-fitting shoes that put pressure on the back of the heel.
- Frequently running on hard surfaces.
- Having an injury or trauma to the ankle joint.
- Having a heel deformity.
- Having an Achilles tendon strain or tear.
- Having flat feet.
- Having a genetic predisposition.
- Being overweight or obese.
- Advancing in age.
The doctor or specialist will perform the necessary tests to determine if the deformity is related to Haglund’s syndrome. During the initial medical examination, the appearance and mobility of the foot will be evaluated. An important characteristic to look for in the diagnosis is the visible protrusion or bump on the back of the heel.
To complete the diagnosis, the doctor may take one or several x-rays. The x-ray, especially in the lateral position of the foot, will show a pronounced bony protrusion or growth in the heel area. The imaging test should also show any calcifications in the Achilles tendon that are causing irritation. Additionally, ultrasound and MRI tests can be done to help determine the state of soft tissues such as tendons, muscles, and bursas. This is where bursitis, or inflammation of the bursa, can be confirmed.
Another test for the diagnosis of Haglund’s deformity is determining the Fowler-Philip angle. This is the angle formed between the lower heel bone and the posterior surface of the heel bone. If the angle measures more than 75 degrees, it indicates the presence of Haglund’s deformity. The larger the angle, the more advanced the stage of the deformity.
The doctor or specialist will perform the necessary tests to determine if the deformity is related to Haglund’s syndrome. During the initial medical examination, the appearance and mobility of the foot will be evaluated. An important characteristic to look for in the diagnosis is the visible protrusion or bump on the back of the heel.
To complete the diagnosis, the doctor may take one or several x-rays. The x-ray, especially in the lateral position of the foot, will show a pronounced bony protrusion or growth in the heel area. The imaging test should also show any calcifications in the Achilles tendon that are causing irritation. Additionally, ultrasound and MRI tests can be done to help determine the state of soft tissues such as tendons, muscles, and bursas. This is where bursitis, or inflammation of the bursa, can be confirmed.
Another test for the diagnosis of Haglund’s deformity is determining the Fowler-Philip angle. This is the angle formed between the lower heel bone and the posterior surface of the heel bone. If the angle measures more than 75 degrees, it indicates the presence of Haglund’s deformity. The larger the angle, the more advanced the stage of the deformity.
Most patients will go home on the same day as their surgery, once the effects of general anesthesia have worn off. However, it’s recommended to wait for about 10-12 hours before doing so, as a drain may be left in place to prevent hematoma formation. Only patients with other significant medical issues will be required to stay overnight for observation of their post-surgery recovery. If all parameters are good the next morning, the patient will be able to return home.
After surgery, patients will leave with a cast or bivalve splint covering the lower leg. This dressing should be kept clean and dry until the tenth day, when it will be removed to allow for the removal of surgical stitches. Patients should not move or remove the dressing themselves.

After 2 weeks following surgery, patients can return to wearing normal shoes and can begin to engage in light activities such as walking. Daily walking, without over-stressing the foot, will help to strengthen the muscles and tendons. Gradually increasing distances is recommended. Running should not be resumed until at least 3 months have passed, while more intense sports activities should be avoided for 9 months.
A physiotherapist will provide the patient with a detailed rehabilitation program. Some people may become frustrated because they feel they are progressing slowly and have lost the athletic abilities they had before surgery for Haglund’s deformity. However, with consistency and patience, many will be able to achieve the expected level. Regaining full strength and balance can take some time.
The appropriate time to resume driving is from the sixth week of recovery, when normal shoes can be worn again. Before driving freely, we recommend doing some tests:
- Sitting in the driver’s seat and, without turning on the car, testing the pedals several times to ensure that we have enough strength in the feet to react in time during driving.
- Driving slowly around the street of the house, without going far, and on less busy streets.
- If the patient feels good control over the vehicle, they can begin to make short trips, not too far from the starting point.
- Having acquired all the necessary skills, the patient can drive freely.
If the car is an automatic, and the surgery for Haglund’s deformity was performed on the left foot, it is likely that the patient can drive earlier than indicated, after the second week. However, as this may involve some risk, it is better to consult with the doctor. Additionally, it is important to consult with the car insurance company and know the conditions to cover any possible accident
The answer to this frequent question will depend on the type of work that the patient does. For those who have a sedentary or desk job, where the operated foot can be kept elevated, they can return to work after the first 2-3 weeks of recovery. If the job is very active, physical, or strenuous, and involves standing or moving around, the patient will need more recovery time before they can return to work. They probably can start from the third month of recovery.
It is not recommended to fly when the surgery is still recent, as this increases the risk of blood clots forming. Blood clots pose a risk of deep vein thrombosis or DVT, which is extremely dangerous for one’s life. It’s recommended to consult with the surgeon about when is the appropriate time to take a flight, as it also depends on the patient’s recovery rate. Furthermore, it’s important to keep in mind that each airline has its own restrictions regarding flying after surgery. Usually, it’s recommended to take a flight only after the first 10 to 14 days of recovery.
After surgery for Haglund’s deformity, the patient will have to make several postoperative visits to the surgeon. These visits aim to observe the healing of tissues and bone, as well as the rehabilitation of the foot.
Let’s see:
- Day 10 (first postoperative visit):
- The cast and stitches are removed.
- A radiograph is also taken to observe the position of the bone.
- If the surgery was performed without debridement or repair of the Achilles tendon, a heel-elevating boot will be placed. This allows for progressive weight bearing, from 10 to 100% over the next 4 weeks.
- However, when the surgery involves debridement of the tendon, patients must continue without exerting pressure on the foot for the next 4 weeks.
- Those who required extensive repair will need a new cast to immobilize for a longer period.
- The surgeon will recommend keeping the foot elevated as needed.
- Sixth week (second postoperative visit):
- When the surgery for Haglund’s deformity did not involve restoration of the Achilles tendon, at this time the patient will have the boot removed and can start walking.
- If there was tendon treatment, the patient will have to start supporting the foot gradually or using the boot, according to the doctor’s guidance in each case.
- The doctor will prescribe certain activities depending on the progress and clinical history of each patient.
- Third month (third postoperative visit):
- Starting from the third month, another visit to the surgeon is made to check the current conditions of the foot.
- At this time, if health conditions allow, the patient will be formally discharged.
- However, the patient will be instructed to continue with physiotherapy and gradually increase the level of exercise.
- Physiotherapy is key to improving the strength and resistance of the foot and ankle.
- Patients must be patient, as a complete rehabilitation may take between 10 and 12 months. Even inflammation may last between 6 and 8 months. The use of compression stockings is recommended to prevent it.
The Haglund’s deformity, in many cases, appears due to wrong habits that patients maintain for years without realizing it. Now we will give some tips to avoid this deformity:
- Avoid frequent use of high heels, shoes that have hard and pointed tips. It is more advisable to use soft shoes and those that do not have a heel.
- Do not run frequently on hard surfaces, such as avenues or sidewalks.
- Avoid running on surfaces that are uphill, as this forces the Achilles tendon.
- People with a very high arch, should use arch supports within shoes, so that the plantar support is more complete.
- Use orthopedic devices that help maintain good posture in the foot.
- Practice stretching exercises that prevent the Achilles tendon from cramping.

What to Expect After Haglund’s Deformity Surgery
When Haglund’s deformity proves to be resistant to all non-surgical remedies, such as changing footwear, anti-inflammatory drugs, and physiotherapy, surgical
Dorsal Heel Spur Surgery – Procedure, Recovery, and What to Expect
Dorsal heel spur surgery is a procedure that alleviates irritating symptoms caused by heel spurs that develop on the back

Bunion on the Little Toe: Causes, Symptoms, and Treatment Options
Many individuals struggle with a bunion on the little toe – this condition can cause unpleasant symptoms and interfere with

How to Treat the Bursitis of a Bunion
When there is a bunion, one of the common complications that can occur is bursitis. This condition is an inflammation

Failed Hammertoe Surgery: Causes, Complications, and Solutions
No matter how experienced a doctor is or how routine the procedure, every surgery poses a certain amount of risk

Floppy Toe After Hammertoe Surgery: Understanding the Phenomenon
Even though hammertoe surgery is a routine, minimally invasive procedure, it still carries a certain amount of risk. One of

Toe Shortening Surgery in Atlanta: A Comprehensive Guide
Foot health is always overlooked until a person starts having difficulties while walking and standing for longer periods of time.

Understanding the Stages of Healing for a Plantar Wart: A Comprehensive Guide
Skin conditions on your feet can be difficult to fully get rid of, which is why it’s so important to

Plantar Wart vs. Callus: How to Differentiate Between the Two
A lot of different skin conditions present themselves in a similar fashion on our feet – rough bumps or patches

Plantar Wart vs. Corn: Understanding the Differences
It’s well-known that plantar warts and foot corns aren’t the same thing – but they still often get confused with

Bone Spur or Bunion: Understanding the Difference
Bone spurs or bunions are different orthopedic issues that can create foot pain and discomfort. Even though they have distinct

Bunion Recovery Week-By-Week Process
Bunion surgery is a highly successful procedure, and most patients recover from it very well and in a short amount